

Alcohol consumption and alcohol-related harm are not distributed equally across society. Some groups face significantly higher rates of alcohol-related illness and mortality than others – even when they drink the same amount, or less, than more advantaged groups. This highlights that alcohol-related harms are shaped not only by how much people drink, but also by the wider social conditions around them.
One possible contributor to alcohol-related inequalities is discrimination. Previous research has shown that people who experience discrimination may be more likely to drink heavily and experience alcohol-related problems. However, most of this research has focused on interpersonal discrimination – for example, being treated unfairly by another person.
To look beyond individual interactions, our team conducted a systematic review focusing instead on structural discrimination: the systemic biases built directly into societal frameworks, institutional practices and public policies. In this blog post, we share the key findings from our review, exploring how these overarching structures affect drinking behaviours and and related outcomes.
What do we mean by structural discrimination?
When people hear the word discrimination, they might think of one person treating another person unfairly. That matters, but discrimination can also operate at a much broader level.
Structural discrimination refers to the ways laws, policies, institutions, neighbourhood conditions, cultural norms and systems of power can create or maintain unequal opportunities for different groups. This might include, for example, racism in housing and criminal justice systems, sexism in employment and reproductive rights policies, or heterosexism in laws affecting LGBTQ+ people.
Put simply, structural discrimination is not just about individual attitudes or behaviours. It is about who has access to resources, protection, safety, power and opportunity, and who does not. Structural discrimination is produced and sustained through institutional and governmental actions and policies – whether intentionally or not.
Why is structural discrimination relevant to alcohol-related outcomes?
Structural discrimination matters for alcohol-related outcomes because it shapes the conditions in which people live, work, socialise, experience stress and access support. These conditions can influence both alcohol use and the harms linked to drinking.
Nancy Krieger's ecosocial theory helps explain this connection. In simple terms, it suggests that people's bodies and health are shaped by the environments and social conditions they live in over time. Experiences such as poverty, unsafe housing, exclusion, social trauma, targeted marketing and poor access to healthcare can become 'embodied' – meaning they can affect people's health in real, biological and emotional ways.
Alcohol-related inequalities are one example of this. In the United States, racist housing policies such as redlining helped create lasting residential segregation. Many minoritised communities were pushed into neighbourhoods with fewer health-promoting resources such as good-quality housing, green spaces, education and healthcare. At the same time, these areas may contain more alcohol outlets and more alcohol advertising, even where demand for alcohol is not higher.
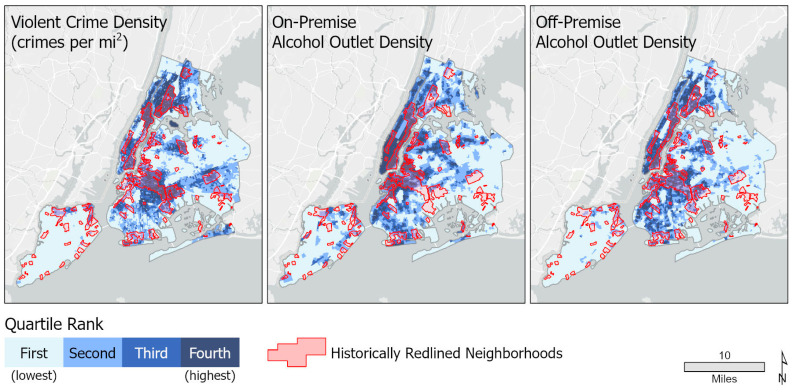
Spatial accessibility index of alcohol outlet density in New York City. Reproduced from Haley et al. (2023), licensed under CC BY 4.0.
Structural discrimination can also create chronic stress and trauma. For example, heavier policing and surveillance in predominantly Black neighbourhoods can place young people under constant pressure. For some, drinking may become one way of coping with the resulting stress.
However, the relationship is not always straightforward. In some cases, structural discrimination may be linked to lower alcohol use. For example, some African Americans may drink less to avoid racist or punitive consequences from wider society or authorities. Strong community norms in some segregated neighbourhoods may also discourage heavy drinking.
Our review: bringing the evidence together
We conducted a systematic review to understand what is currently known about the relationship between macro-level structural discrimination (including all studies examining discrimination beyond the individual or interpersonal level) and alcohol outcomes. We were interested in two broad types of outcome: alcohol consumption, such as drinking frequency or heavy episodic drinking, and alcohol-related health harms, such as alcohol use disorder, liver disease or alcohol-attributable mortality.
We searched four academic databases, alongside grey literature and reference lists, for studies published between 1990 and August 2024. To be included, studies had to use quantitative measures of discrimination at a macro level – for example, state policies, neighbourhood segregation, or country-level gender equality indicators – rather than only individual reports of unfair treatment.
What did we find?
In total, we included 25 studies. Most were conducted in the United States. The most commonly studied form of structural discrimination was racism, followed by sexism, heterosexism, and studies considering more than one form of discrimination at the same time.
The findings were mixed. There was no single, straightforward pattern where structural discrimination was always associated with increased or decreased drinking across all groups and outcomes.
Instead, the relationship depended on several things: the type of discrimination being studied, how it was measured, which population was exposed, and which alcohol outcome was examined.
Structural racism
Structural racism was the most frequently studied form of discrimination in the review, with most studies focusing on racial segregation in schools or neighbourhoods. Findings were inconsistent: some studies linked segregation to higher levels of some drinking outcomes among Black Americans, while others found no association or lower alcohol use in some segregated settings.
This does not mean structural racism is harmless. Rather, different mechanisms may operate in different contexts. Segregation may increase harm through neighbourhood disinvestment, alcohol outlet density, stress and reduced access to protective resources. However, some predominantly Black communities may also have stronger collective norms, religious involvement or family support that discourage heavy drinking. Fear of racially biased policing or punishment may also reduce drinking in public or reporting of drinking.
Studies that looked beyond segregation found some evidence that other forms of structural racism, such as racial inequalities in poverty and incarceration, may be linked to increased alcohol use and harm among Black and Hispanic populations.
Structural sexism
Studies of structural sexism often used composite measures of gender inequality, including indicators of income, employment, political representation, reproductive rights and violence policy.
Findings were also complex. Some evidence suggested that women may be more likely to drink at all as gender equality increases, possibly reflecting changing gender roles, greater participation in public life, or shifts in norms around women's drinking. However, this does not mean sexism is protective. Some studies linked structural sexism to higher levels of risky drinking and alcohol-related mortality, while findings for heavy episodic drinking and drinking frequency were mixed.
This highlights that lower drinking does not necessarily mean better health or greater equality. If women drink less in highly sexist contexts because their freedom, income, public participation or autonomy are restricted, that is not a public health success.
Structural heterosexism
Evidence on structural heterosexism was more limited and mainly focused on policy environments affecting LGBTQ+ people, such as legal protections, marriage bans and broader state-level policy climates.
Overall, there was some evidence that more discriminatory policy environments were associated with alcohol use disorder among sexually minoritised groups, and with high-intensity drinking among sexual minority men. However, the number of studies was small, and findings varied across outcomes and subgroups.
Intersectional discrimination
Only a few studies considered intersectionality, i.e. considered the combined influence of multiple forms of structural discrimination simultaneously. This is an important gap, because people do not experience racism, sexism, classism, heterosexism or other systems of power in isolation.
The available evidence suggests these systems may interact. For example, in studies of Black sexual-minority men, structural racism was associated with heavier drinking, and this association appeared stronger in states with more anti-LGBTQ+ policies. In other words, one form of structural discrimination may amplify the harms of another.
What does this mean?
Efforts to reduce alcohol harm need to look beyond individual behaviour change. This review suggests that structural discrimination can shape alcohol use and alcohol-related harm in complex ways. This has three key implications:
Dismantle structural discrimination
Efforts to reduce alcohol harm should include action to dismantle structural discrimination. Where discrimination is linked to worse alcohol outcomes, it points to systems that need to change – such as discriminatory policing, judicial bias and the wider drivers of incarceration inequities.
Address the harmful effects of discrimination on drinking
We need to address the harmful effects of discrimination on drinking. This could include, for example, improving access to alcohol treatment and support in affected communities, reducing targeted alcohol marketing, or offering brief alcohol interventions in criminal justice settings.
Protect at-risk groups while promoting equity
Some groups, such as employed women, may drink more in contexts of reduced gender discrimination. The response should not be to treat gender equality as the problem, but to support these groups (e.g. through targeted interventions) while continuing to promote equity.
Overall, reducing alcohol-related inequalities means tackling discrimination directly, reducing the harms it causes, and supporting equality in ways that protect health.
A few caveats
There are some important limitations to keep in mind from our systematic review:
- Small evidence base: Despite searching broadly, we found only 25 studies. Most came from the United States, meaning we know much less about these relationships in other countries, including the UK.
- Inconsistent measures: The studies used many different measures of structural discrimination and alcohol outcomes, making it difficult to compare findings directly. For example, one study might measure structural racism through school segregation, while another uses incarceration gaps or income inequality. These are related, but they are not the same thing.
- Focus on consumption over harm: Most studies focused on alcohol consumption rather than alcohol-related harm. This is important because groups can experience greater alcohol harm even when they drink similar or lower amounts. More research on outcomes such as alcohol-related hospital admissions, liver disease and mortality would help us better understand how structural discrimination contributes to health inequalities.
- Isolated variables: Many studies examined only one form of discrimination at a time. Future research needs to better capture how systems of oppression overlap and interact.
Where next?
There is still much to learn about how structural discrimination shapes alcohol use and alcohol-related harm. Most research so far has focused on racism and sexism, but other forms of discrimination – such as ableism, ageism and xenophobia – also need more attention.
Future research should also look more closely at how different systems of discrimination overlap. People do not experience racism, sexism, class inequality, ableism or other forms of disadvantage in isolation, so studies need to better capture how these systems combine across people's lives.
Better measures are also needed. Rather than looking at single policies or institutions in isolation, researchers should develop broader measures that capture discrimination across multiple areas, such as housing, employment, criminal justice, healthcare and policy environments.
Finally, future studies should do more to understand why these links exist, not just whether they exist. This means looking at long-term patterns, testing possible pathways, and focusing not only on alcohol consumption, but also on alcohol-related harms. Understanding these processes more clearly can help identify where policy and public health action may be most effective.
Contact and further information
This blog post was based on the following paper:
Bright S, Buckley C, Holman D, et al. (2025) The association between macro-level structural discrimination and alcohol outcomes: A systematic review Social Science & Medicine DOI: https://doi.org/10.1016/j.socscimed.2025.118596
The map used in this post ('Spatial accessibility index of alcohol outlet density in New York City') was reproduced from the following paper under a Creative Commons Attribution (CC BY) license:
Haley SJ, Jardine SJ, Kelvin EA, Herrmann C, Maroko AR (2023) Neighborhood alcohol outlet density, historical redlining, and violent crime in NYC 2014–2018 International Journal of Environmental Research and Public Health DOI: https://doi.org/10.3390/ijerph20043212
For further information about this research please contact Sophie Bright at the University of Sheffield.